Vitamin K2 MK-7, 3 Years: 244 Postmenopausal Women Slowed Bone Density Loss
Vitamin K2 (MK-7, menaquinone-7) data has accumulated over 3-year trials showing it slows bone density and strength decline in postmenopausal women. 244 healthy postmenopausal women taking MK-7 180 μg/day for 3 years showed significantly reduced age-related bone density and strength loss.
Osteocalcin and Bone Mineralization
Vitamin K2’s mechanism centers on osteocalcin (OC), a protein osteoblasts produce that drives bone mineralization (calcium-phosphorus binding).
Osteocalcin is made in an under-carboxylated state. Vitamin K serves as the cofactor in carboxylation, converting osteocalcin into the active form capable of binding calcium to bone. Without vitamin K, osteocalcin is manufactured but cannot build bone.
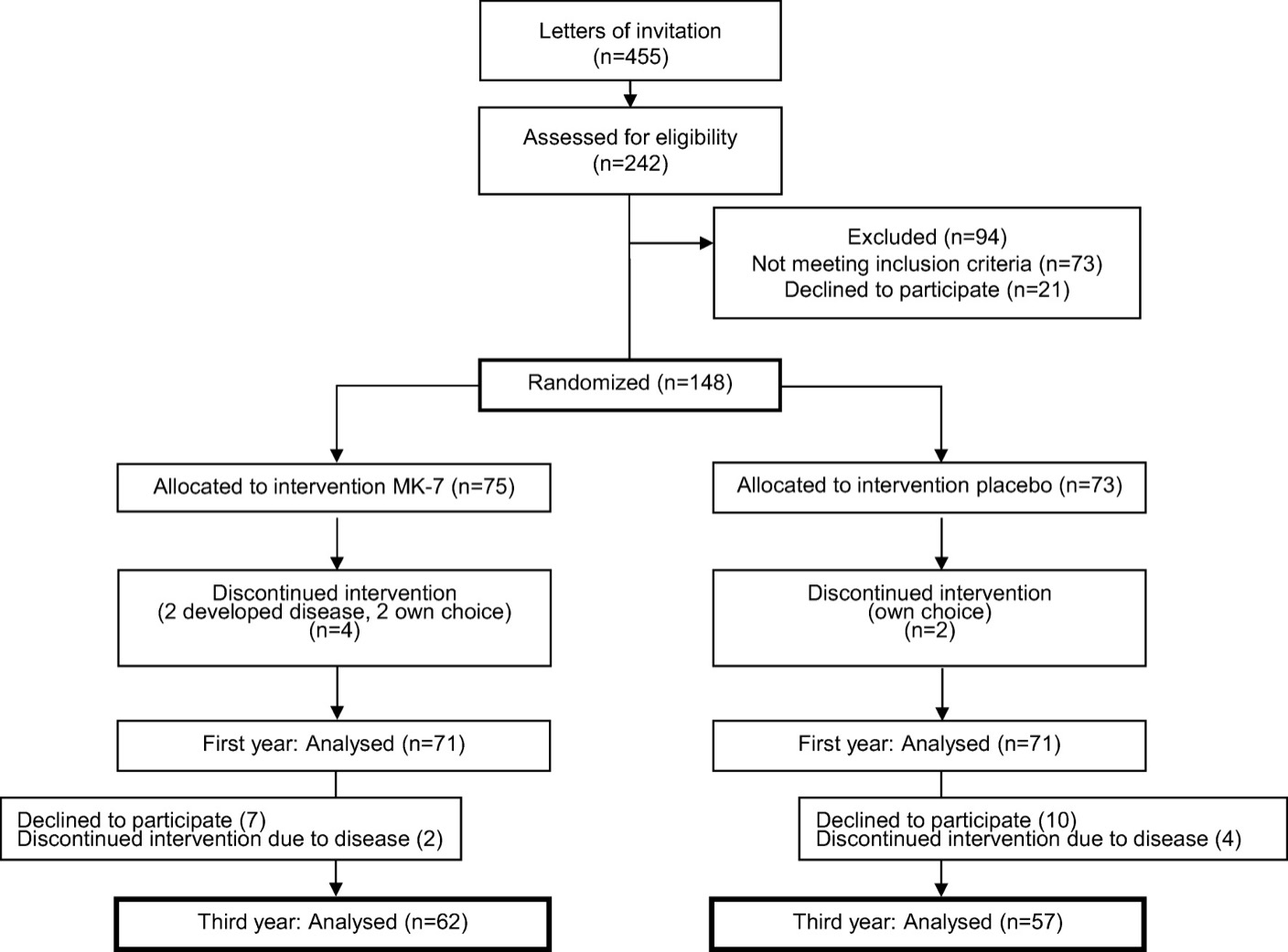
High-Dose 3-Year Trial
In postmenopausal women with osteopenia (142 participants), MK-7 375 μg/day for 3 years reduced under-carboxylated osteocalcin by 65.2% at 1 year (vs 0.03% placebo, p<0.01). Both groups took vitamin D3 38 μg and calcium 800 mg.
Vitamin K2 functions as the cofactor that maximizes calcium and vitamin D effects.
Dietary Sources
K2-rich foods:
- Natto: ~900 μg per 100 g (MK-7)
- Korean fermented soy paste (cheonggukjang): ~500-800 μg per 100 g
- Hard cheese (Gouda, Parmesan): ~50-80 μg per 100 g
- Egg yolk: ~15 μg per egg
- Grass-fed butter: ~15 μg per 100 g
Natto dominates as an MK-7 source. A 30-50 g serving provides nearly the 180 μg clinical dose.
The D3 + K2 + Magnesium + Calcium Quadrangle
Modern bone strategy uses four ingredients, not one:
- Vitamin D3 2,000 IU: calcium absorption
- Vitamin K2 180-375 μg: precise bone calcium placement
- Magnesium 300 mg: vitamin D activation + bone structure
- Calcium 1,000-1,200 mg: raw material
The calcium paradox: without K2, calcium deposits in blood vessels and soft tissue instead of bone, potentially raising cardiovascular risk. This drives D3+K2+calcium combinations as the new standard.
Dosing and Forms
- Dose: MK-7 180-375 μg/day
- Timing: with fat-containing meals (fat-soluble)
- Duration: minimum 1 year, ideally 3+ years
- Forms: capsule or softgel. Plant-derived (natto ferment) MK-7 preferred
Cardiovascular Benefit
K2 acts on cardiovascular health too. The Rotterdam Study showed the highest MK-7 intake group had 57% lower cardiovascular mortality. The hypothesis: K2 prevents vascular calcification where calcium deposits in arteries.
Cautions
- Warfarin users: K2 interferes with warfarin action. Clinician consultation mandatory
- NOAC/DOAC: no interaction with vitamin K
- Pregnancy/lactation: dietary intake safe; high-dose supplements require clinician guidance
Meaning for Women
Women post-menopause lose 1-2% bone density per year, with osteoporosis and fracture risk rising sharply after 60. Natto consumption varies regionally, making dietary K2 access limited for many, and 180 μg/day supplementation becomes the pragmatic strategy.
Calcium and vitamin D supplements are mainstream, but K2 remains underappreciated. As 2020s long-term trials accumulate, K2 is being repositioned as the missing piece in bone health supplementation.